Last Updated on 9th May 2026 by Caroline Haye

Ruxolitinib and beyond
If you, or someone else in your life, have vitiligo you probably already know that the first ever anti-vitiligo drug to hit the market recently received approval for NHS use in the UK. And you may also appreciate the monumental step forward this achievement represents. In fact, it is the culmination of decades of sustained effort by literally thousands of individuals and teams in creating awareness, overcoming ignorance, raising funds, conducting painstaking scientific research and jumping through countless political, regulatory, fiscal and administrative hoops in pursuit of a cure for this distressing and long neglected condition.
As the first dedicated pharmaceutical for the repigmentation of non-segmental vitiligo, ruxolitinib cream (Opzelura) brings new hope to millions of patients here, as well as in the US and EU where it received approval faster than in the UK. And, more than that, it has paved the way for other treatments that will give people with vitiligo more personalised options, real choice and better outcomes in the future. So, momentous as NICE approval of ruxolitinib for vitiligo is, my prediction is that life after Opzelura will be more exciting still.
A quick recap of the Opzelura story
To recap the story so far, Opzelura is the brand name for the 1.5% ruxolitinib cream approved for the topical treatment of non-segmental vitiligo. Ruxolitinib itself is a type of drug called a JAK inhibitor, so named because it reduces inflammation by inhibiting JAK1 and JAK2 enzymes. (JAKs – short for Janus kinase – are enzymes that play a key role in the inflammatory process.)
An oral form of ruxolitinib was originally used in the treatment of a rare blood cancer called myelofibrosis (MF). Researchers later transitioned ruxolitinib from an oral myelofibrosis treatment (Jakafi) to a topical vitiligo treatment by identifying that the same JAK1/JAK2 signalling pathway causing runaway inflammation in blood cancers also drives the autoimmune destruction of melanocytes in vitiligo. And so – following a rigorous process of clinical trials and regulatory review – Opzelura is finally available to vitiligo patients and is officially the first licensed, NHS-approved treatment for the underlying cause of the condition.
Opzelura results so far
First, the good news…
When it comes to a multifactorial, treatment-resistant condition like vitiligo, any approach that produces measurable results on a fairly consistent basis is cause for huge celebration. And Opzelura appears to be doing exactly that.
Patients so far are achieving the most significant repigmentation on their face, neck and chest and on those areas of skin with higher numbers of hair follicles. About 30% of patients are experiencing a 75% improvement in facial vitiligo. And the cream is currently achieving high satisfaction rates of up to 79% after six months of use. So, it’s no wonder that Opzelura is attracting so much attention in the vitiligo community.
Now, the bad news…
Opzelura is expensive to buy privately and not everyone with vitiligo in the UK will have access to it on the NHS. It will only be offered to adults and children over twelve with non-segmental vitiligo, and only as a second‑line treatment. (This is when the use of first‑line topical treatments, such as topical corticosteroids or calcineurin inhibitors, have been ineffective or are unsuitable.) Even then, I am hearing reports of patients being denied Opzelura anyway due to its high cost and the pressure on the NHS to save money.
It is also important to recognise that, as with all pharmaceuticals and natural remedies alike, success is not guaranteed. In common with most vitiligo therapies, results vary considerably and they do take time (e.g. six months or more). It is a slow process that requires consistent daily application and patience. Plus, side-effects are always a risk to bear in mind, the most common (affecting up to one in ten people) being acne at the application site and dry skin. In addition to these drawbacks, the application of Opzelura is restricted to just ten percent of the body’s surface area only, which is obviously a significant limitation for those with widespread vitiligo.
What comes next?
Following such a significant breakthrough in the medical treatment of vitiligo, you might be wondering if researchers will be resting on their laurels or turning their attention to other conditions. But the opposite seems to be true. They are, in fact, working on improving the efficacy of JAK inhibitors further, as well as incorporating them into combination therapies, and developing new formulations in order to overcome current limitations. So, it seems that we can look forward to some significant improvements to Opzelura, as well as the development of other next-generation therapies over the coming years.
Combination therapies
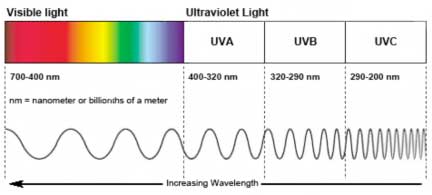
Research indicates that combination therapies for vitiligo and many other conditions have a synergistic effect, producing better results than any single approach in isolation. For example, pairing Opzelura with other treatments (specifically narrowband UVB phototherapy) produces superior, faster, and more extensive repigmentation than using the cream alone.
Similarly, the synthetic hormone afamelanotide (brand name Scenesse) is designed to accelerate repigmentation of vitiligo, also in combination with NB-UVB phototherapy. (Clinuvel is currently in Phase 3 trials of this subcutaneous implant.)
Improved formulations for next generation topical JAK inhibitors
Whereas the current version of Opzelura is a JAK1/2 inhibitor, there are new, softer JAK inhibitors currently in development. So called “soft” JAK inhibitors are more selective in that they are highly effective at the application site (e.g. on vitiligo lesions) but rapidly inactivated upon entering the bloodstream, thereby minimising systemic side effects. The hope is that these improved creams will remove the ten percent body surface area restriction and provide better results on difficult areas like hands and feet.
Oral (systemic) alternatives
For patients with widespread vitiligo, it would be impractical as well as unsafe to apply the current topical version of Opzelura to all affected areas of skin. So work is progressing on oral JAK inhibitors, such as upadacitinib and povorcitinib (currently in phase 3 trials), which will work systemically and which researchers hope will provide more comprehensive treatment options.
“Durable Remission” drugs
A major focus for researchers now is to develop treatments that go beyond JAK inhibitors and beyond simply managing symptoms. Specifically, they are working on IL-15 inhibitors (such as TEV-53408) which will target tissue-resident memory T cells, aiming for a “reset” of immune memory to achieve lasting repigmentation and prevent lesions from returning.
In addition to the above, phase 2 trials are due to start imminently of another type of drug called a CXCL10 inhibitor (e.g. EB06) which aims to interrupt the immune-mediated destruction of melanocytes, thereby preventing depigmentation before it starts.
Photocil
Research is also ongoing into the use of an ingenious topical cream called Photocil, which filters natural sunlight to allow narrowband UVB to reach the skin whilst blocking harmful wavelengths. The idea of this is that patients will be able to have the benefits of phototherapy without the need for expensive home equipment or hospital visits. As a stand alone treatment, this would presumably be no more effective than current phototherapy options, although much more convenient. But it potentially brings with it a significant benefit in making combination therapy much simpler to apply.
Bacterial therapy
And finally, there is a completely different area of research that, in my opinion, promises more advantages with fewer drawbacks than all the others: bacterial therapy. Recent research indicates that vitiligo has a strong association with gut microbiota imbalance (dysbiosis), which contributes to oxidative stress in the skin and immune dysfunction. Evidently, vitiligo patients have significantly lower microbial diversity, a lower Bacteroidetes-to-Firmicutes ratio and a decrease in beneficial short-chain fatty acid (SCFA)-producing bacteria than the norm.
So this raises the possibility that enriching and rebalancing an individual’s microbiome might prove to be a safe, effective – and literally organic -way of cutting vitiligo off at its roots. (And, in my opinion, this is the most exciting and promising strategy of them all. I say this because it seems to involve correcting an imbalance in the body’s natural flora instead of using drugs to interrupt biological processes… A gentler approach, which presumably would have few, if any, unwanted side effects.
To summarise
Whilst Opzelura definitely represents a major milestone in vitiligo treatment (delivering 75% or greater improvement in facial vitiligo for a significant number of people, especially when used for 1 – 2 years or more), it really is just the first of many new therapies that are in the pipeline. The goal now is to develop treatments that are faster-working, longer-lasting and more effective, especially in more resistant, non-facial, areas. So, it’s exciting to know that we can expect a succession of new treatments to emerge in the next few years. Not only will this provide more choice (and greater hope) for patients, but it will also increase the options for doctors to be able to match the right treatment strategy to the right individual, given that vitiligo is not a one-size-fits-all kind of condition.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
6 thoughts on “Life after Opzelura”
I achieved the greatest repigmentation using Boost, Five a Day, and NB UVB. 80% of full facial repigmentation! But this was also when my gut infection, SIBO, was completely in remission. So I think the microbiome is a key stepping in healing.
The only other treatment that worked faster is the Dead Sea treatment with Dr Schallreuter’s pseudocatalase cream. Achieved 60% full body repigmentation that lasted 20 years. Lost some pigment when I was exposed to mold in a water damaged building and got very sick.
Thanks very much for your feedback. It’s always very encouraging to hear what has worked for others. And I’m really happy to know that both of these approaches worked so well for you.
Hello. I have a segmental vitiligo and I’m wondering if there are any researches for it. I have the feeling that they only focus on non-segmental-vitiligo. Having said that, I’ve tried the cream for less than a month and go a very bad cold. I don’t know if it was a side effect of the treatment or just bad luck.
Thanks for raising this point. You are right that vitiligo research seems to have focussed more on NSV than segmental, maybe because it is a lot less common and tends to be more stable. Having said that, there are several surgical treatment that can get pretty good results with stable cases of segmental vitiligo. And there are several new approaches under development at the moment, specifically aimed at segmental vitiligo. In fact, you have inspired me to cover this in a future post. So thank you for that!
As for your bad cold, yes – I am guessing it could well be because Opzelura can increase the risk of infections because of the way it acts on the immune system. I’m not a doctor of course (so please check with yours), but my understanding is that it is only for use on non-segmental vitiligo. So it is probably unsuitable for your vitiligo. I hope you feel better soon.
Thank you so much for this post, Caroline. Bacterial therapy is really interesting. Always a good idea to use natural treatments, I figure. I take dietary supplement to keep my gut bacteria ‘happy’. Here´s some more information on this topic, although the article does not specifically refer to our condition:
https://supersynbiotics.se/en/maghalsa/gut-flora/how-does-your-gut-flora-affect-your-skin/?utm_source=Klaviyo&utm_medium=email&utm_campaign=Hudens+h%C3%A4lsa+b%C3%B6rjar+i+tarmfloran&_kx=8Xb4qrKJvED8KdnZWI821nQvlHTQY9Jay2Bz5M_cTuc.SmbJL8
Warmest spring greetings,
Gösta
Many thanks for this, Gösta. Yes – it is a huge and fascinating topic and one that I really hope will eventually provide a safe and lasting treatment for all chronic skin conditions. (Spring greetings to you too… it’s not very warm here yet, but we live in hope!)